Social Work Presentation
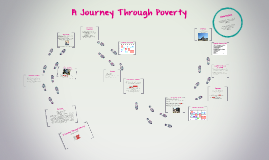
Transcript: Schedule & Bus Routes This situation is ideal, but in reality, Charlotte's outcome could have been very different. Income Conclusion Food Stamps & Insurance Daughters of Charity & Goodwill Job Search Continued - Insurance: $95 fee for 2014 year November 2, 2013: Begins job search with the help of the halfway Begins preparations for interview November 18, 2013: Gets first job at McDonalds - $184/week with taxes (25 hours/week) - 1025 Main Street November 19, 2013: Training and first day of work Weekly Grocery List Recovery Network of Programs - First Step Detox Medically monitored in-patient detox unit for alcohol, opiates, and benzodiazepines Used evidence-based treatment Has trained clinical staff Has medical interventions tailored to individual needs Job Search - Prepaid TracPhone: Samsung S380C Reconditioned - $9.99 60 minutes per month- $19.99 November 22, 2013: Gets second job at Merchandise Mart - $184/week with taxes (25 hours/week) - 3135 Park Avenue November 23, 2013: Training and first day of work Expenses = $ Charlotte's Timeline - Bus Voucher: $70 / month for ZipTrip bus pass - unlimited use According to the NDA, 40-60% of those with an addiction relapse at least once. April 10, 2013: Arrested for possession of marijuana April 14, 2013: Court date where plea bargain signed→ Court Ordered Rehab May 4, 2013: In Halfway house Regional Network of Programs; First Step Goodwill: 165 Ocean Terrace, Bridgeport, CT 06605 - Buys: spatula, lamp, other furniture, clothes for work (pants, blouses, jacket, etc) AA Meetings - Rent: $450 / month A Journey Through Poverty Elizabeth Broderick Chelsea Geremia Rachel Hurton Jessica Wyszynski Wednesdays - 7pm United Congregational Church 877 Park Ave. Open Big Book Meeting A Journey Through Poverty Name: Charlotte Small Age: 40 years old Marital Status: Single History: Charlotte has a high school education, a history of sexual abuse throughout her childhood, and an addiction to drugs and alcohol that began when she was 15 years old. After being arrested for marijuana, she signed a plea which led her to court ordered rehab. Currently she is living in a halfway house where her time is coming to an end. She is a smoker with a sporadic work history and has to continue checking in with a probation officer, stay in recovery, and attend AA meetings. $368/week, $1,472/month After taxes taken out Working two jobs 25 hours a week each job (50 hours a week total) Paid minimum wage After expenses, ~$ 300 left a month to save Insurance: ConnectiCare Charlotte does not qualify for any SNAP benefits due to her monthly income of $1, 472 APARTMENT Schedule & Bus Routes SNAP: Supplemental Nutritional Assistance Program - Groceries, Toiletries, & Cigarettes: $500 / month ConnectiCare Solo $258/month Due to high cost, she chose NOT to purchase insurance and instead will pay the $95/year fee for being uninsured Due to her yearly income of $17,664, she does not qualify for the EITC which cuts off at $14,340 for single individuals Daughters of Charity: 1490 North Avenue, Bridgeport, CT 06604 - Rescue Mission- Furniture & Clothing Bank - Receives: mattress, pots, pants, utensils, plates, bed linens, towels, table, chairs, couch, etc HALFWAY HOUSE History November 20, 2013: Begins search for apartment with the help of halfway house - Decides to room with another woman leaving rehab, named Emily December 1, 2013: finds apartment on Iranistan Ave - Puts down first and last month's rent of $900 December 18, 2013: Moves into apartment - Goes to Daughters of Charity Found in: Stop & Shop and Goodwill Including: bananas, milk, cereal, soup, bread, peanut butter Required as part of plea bargain Set in Bridgeport, CT Finding a Place to Live